
Study Populations & Recruitment Staff
Jump down to:
- Study populations
- Recruitment Staff
Study populations
PRIMERO
Background
Why do some children with respiratory viral infections go on to develop severe respiratory illness, childhood wheeze, and asthma? Decades of studies have demonstrated the strong relationship between severe early-life viral respiratory illnesses and the development of childhood wheeze and asthma, particularly early-life respiratory illnesses caused by respiratory syncytial virus (RSV) and human rhinovirus (HRV). However, most people affected by respiratory viruses are resilient to severe illness, recurrent wheezing, and asthma.
We believe there is a complex interaction between genetics, viral species, and environmental exposures in determining asthma risk.
The Puerto Rican Infant Metagenomic and Epidemiologic study of Respiratory Outcomes (PRIMERO), Puerto Rico’s first birth cohort, was designed to illuminate the early-life origins of asthma and other respiratory conditions.
We are recruiting 3,000 mothers and their newborn infants in Puerto Rico; following the infants for the first five years of life. We will track infants’ respiratory illnesses and determine how early-life viral infections change the trajectory of the infants’ developing airways.
Why Puerto Rico
Puerto Ricans are among the most severely affected populations by asthma in the world. They have the highest childhood asthma morbidity and mortality rates, and the lowest response to common asthma medications such as albuterol. Additionally, Puerto Ricans are disproportionately affected by early-life respiratory illnesses such as pneumonia, bronchitis, and RSV. Interestingly, Puerto Rico has an RSV season that is year-round whereas the mainland United States only reports a 20 week season.
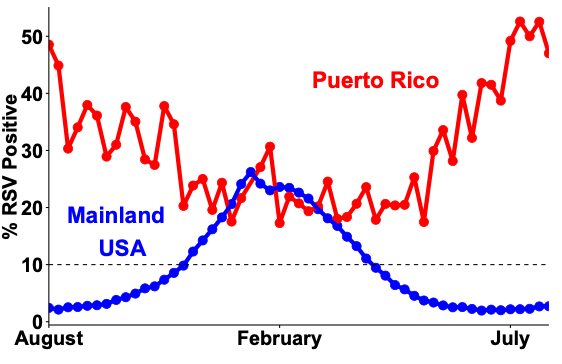
Respiratory syncytial virus (RSV) season in Puerto Rico (red) and the mainland United States (blue). RSV season begins when 10% or more of RSV tests are positive.
The PRIMERO Team

The chief architects of PRIMERO, left to right, Sam Oh, PhD, MPH; José Rodríguez Santana, MD FAAP, FCCP; Max Seibold, PhD; and Esteban G. Burchard, MD, MPH.
PRIMERO is a collaborative effort between Centro de Neumología Pediátrica (CNP), University of California San Francisco (UCSF), and National Jewish Health (NJH). CNP is in charge of recruitment, assessment, and follow-up of patients. UCSF will act as a biobanking and data coordination center and perform genetic analyses on PRIMERO samples. NJH will be the hub for RNA-seq and airway biology analyses.
Recruitment Strategy

Recruitment will begin before the infant is born in the OB/GYN offices at CNP. Mothers will be approached with informational packets and consent for sample collection and study participation. At the time of the baby’s birth, PRIMERO staff will assess the eligibility of the infant and collect cord blood samples. Two to three days later, while the infant and mother are under care in the maternity ward, PRIMERO staff will reaffirm consent to participate, administer a questionnaire, and collect samples from both mom and baby. The infant will be followed by PRIMERO staff for the first five years and contact will be made between PRIMERO staff and participants at respiratory illness visits and yearly check-ups.
The GALA and SAGE Studies

The GALA and SAGE studies investigate the interactions of genetic and environmental risk factors that influence asthma and asthma-related traits among children and adolescents.
Our gene-environment study of asthma in minority children is the largest in the United States. We recruited more than 9,000 participants with detailed measures of asthma, pulmonary function testing, bronchodilator drug response, genome-wide SNP data, detailed measures of air pollution, exposure to tobacco smoke, socioeconomic status, discrimination, and acculturation. These study populations consist of four independent recruitment efforts:
- Genetics of Asthma in Latino Americans (GALA I study)
- Genes-environments & Admixture in Latino Americans (GALA II study)
- Study of African Americans, Asthma, Genes, & Environments (SAGE I)
- Study of African Americans, Asthma, Genes, & Environments (SAGE II)
GALA I is a family-based Latino study. SAGE I is a parallel case-control study in participants ages 8-40. Both GALA II and SAGE II are parallel case-control studies using similar protocols and questionnaires as described in Nishimura (AJRCCM 2013). Subjects were recruited from five urban study centers across the mainland U.S. and Puerto Rico. We have genome-wide SNP genotypes on all participants and air pollution and tobacco data on 5,138 subjects. Latino children were recruited from the San Francisco Bay Area, Chicago, Houston, New York City, and Puerto Rico. African American children were recruited from the SF Bay Area.
Participants were 8-21 years old at time of recruitment and had physician-diagnosed asthma. Healthy controls had no reported history of asthma or allergies, use of medication for allergies, or any symptoms of wheezing or shortness of breath during their lifetime. All subjects with asthma must have had asthma symptoms and/or asthma medication use within the last two years, with no history of other lung or chronic non-allergic illnesses; active smokers were excluded. Parents and grandparents must have self-identified as Latino (GALA I & II) or African American (SAGE I & II).
We have detailed clinical measures (bronchodilator response testing, spirometry, exhaled nitric oxide, skin pigmentation, skin prick testing, complete blood counts, and IgE measurements), biologic specimens (whole blood, RNA, DNA, and nasal epithelia), geocoded air pollution measures, and questionnaire-based information regarding social and environmental risk factors. Genome-wide SNP genotypes are available for all GALA II and SAGE participants from the Affymetrix 6.0 array or Axiom LAT1 array (Affymetrix, >800,000 SNPs) for GALA II and SAGE II.
Number of individuals enrolled in our studies
|
Study |
Ethnicity |
Total |
Cases |
Controls |
Parents |
|---|---|---|---|---|---|
|
GALA I |
Hispanic/Latino |
2499 |
707 |
378 |
1414 |
|
GALA II |
Hispanic/Latino |
4885 |
2233 |
2478 |
174 |
|
SAGE I |
African Americans |
494 |
308 |
186 |
NA |
|
SAGE II |
African Americans |
1736 |
958 |
778 |
NA |
|
Total |
Hispanic/Latino or African Americans |
9614 |
4206 |
3820 |
1588 |
Poor response to therapies contributes to racial/ethnic disparities in asthma morbidity and mortality. Therefore, one of the main goals of the lab is to study the response to albuterol, the most commonly prescribed asthma medication in the world and the mainstay of acute asthma management across all racial/ethnic groups. We have a large collection of DNA samples from 4,111 participants with asthma with measurements of bronchodilator response (BDR).
Total number of participants with asthma included in GALA and SAGE studies of bronchodilator response (BDR)
|
High responders |
Low responders |
|
|---|---|---|
|
African Americans |
601 |
617 |
|
Mexicans |
319 |
642 |
|
Puerto Ricans |
725 |
631 |
|
Other Latinos |
221 |
355 |
|
Total |
1866 |
2245 |
|
High responders and low responders are defined as BDR ≥8% and BDR <8%, respectively. BDR ≥8% is well correlated with asthma and wheezing in children. |
||
Recruitment staff
The Asthma Collaboratory has a full-time clinical recruiter who is trained in performing spirometry, phlebotomy, and clinical characterization, and in administering clinical questionnaires. In addition, we have a clinical coordinator who organizes all clinical recruitment inside and outside UCSF. Together, the recruiter and coordinator ensure that recruitment and phenotype procedures are standardized across all sites. Both will travel to all our clinical sites and provide standardized training on phenotype characterization and questionnaire administration.