Type 1 Diabetes (T1D) affects 20.8 million people worldwide and this number is expected to increase to 32.1 million by 2040. T1D is an autoimmune disease in which the immune cells attack the insulin producing beta cells in the pancreas. Due to this, a type I diabetic has very few functional beta cells due to which they are unable to produce enough insulin and correct blood glucose levels. Current treatment includes providing an exogenous supply of insulin through insulin pumps and injections. However, due to patient compliance and insulin dependency, this is not an ideal treatment option. Islet transplantation using macroencapsulation devices is an alternate strategy that is promising. In this strategy, the original beta cells that have been destroyed in the patient are replaced with donor cells, and these cells are placed in an immune-isolating device that can protect the donor cells from the autoimmune response. However, currently, there is a lack of a safe and effective technology for transplanting these cells within patients.
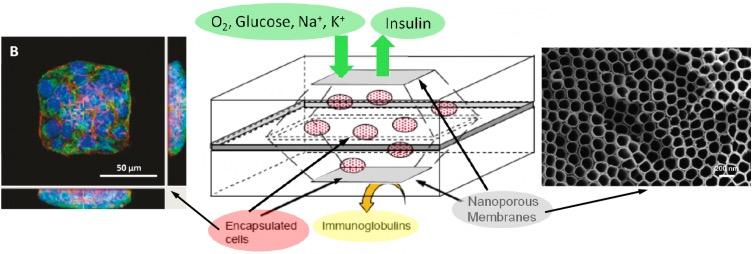
The Desai lab has fabricated a porous thin film cell encapsulation device that can support and protect that encapsulated beta cells. This device is biocompatible, retrievable, and the semi-permeable membrane permitting the entry of nutrients and small molecules while still protecting the encapsulated cells from the host immune system. We have shown that this device is able to support encapsulated stem cell derived insulin producing cells for up to 6 months when transplanted near the kidney or liver. However, for a more translational approach, current efforts are focused on implanting these devices in the subcutaneous space - an implant site that is easily accessible but has inherently low vasculature. Due to this, we are looking for various ways to enhance our current devices such that we can provide additional support to the cells while the device is integrated into the body.
Recently, we published our efforts on the incorporation of a nutrient releasing internal compartment that provides essential amino acids to the encapsulation cells for up to 2 weeks. The addition of the internal compartment has shown to increase graft survival by ~30%, when implanted in the subcutaneous space.
- Providing structural support to encapsulated cells within the device
- Modulating local immune environments to limit inflammation and foreign body response
- Addressing hypoxia within the device
Point(s) of contact: Dr. Bhushan Kharbikar, Gauree Chendke

In collaboration with the Tang Lab.